Intraperitoneal chemotherapy and its use in cancer treatment:
Two types of intraperitoneal chemotherapy are in use:
Α. hyperthermic intraperitoneal intraoperative chemotherapy (HIPEC)
Β. early postoperative intraperitoneal chemotherapy under normothermia (EPIC)
The rationale for the use of intraperitoneal chemotherapy is based upon the fact that there is a physiologic anatomic barrier between plasma and peritoneal cavity that does not permit rapid absorption of large molecular weight substances that are instilled in the peritoneal cavity. Most of the cytostatic drugs are large molecular weight substances that are confined at the peritoneal surfaces and act for long and intensively while they are slowly absorbed in the systemic circulation. As a consequence, they have the ability to eradicate the peritoneal implantations. One disadvantage of the method is that intraperitoneal chemotherapy can destroy seedings that are less 2-3mm in their largest diameter. It is obvious that the role of cytoreductive surgery is crucial because the less the residual tumor the better the effect of intraperitoneal chemotherapy is.
Α. Hyperthermic intraperitoneal intraoperative chemotherapy (HIPEC)
After tumor resection four drains are usually placed in the peritoneal cavity (two under the hemidiaphragms and two in the pelvis). The device is usually comprised of one or two roller pumps, one thermostat, one heat exchanger and an extra corporeal circuit. The perfusate flow is controlled as well as the heat exchanger adjusts the temperature of perfusate, by circulating water at a desired temperature. The temperature in the abdominal cavity is maintained at 42.5-430C and is the mean temperature of the thermistors that are placed in the abdominal cavity.
Usually Normal saline or Ringer’s lactate or peritoneal dialysate 1.5% glycose are used as carriers of the cytostatic drugs.
Three different ways of perfusion are being used:
-
the closed abdominal technique
-
the semi-closed abdominal technique
-
the open abdominal technique (Coliseum technique)
The open abdominal technique (Coliseum technique) seems to be superior because the surgeon can easily distribute manually both the temperature and the cytostatic drugs at the peritoneal surfaces.
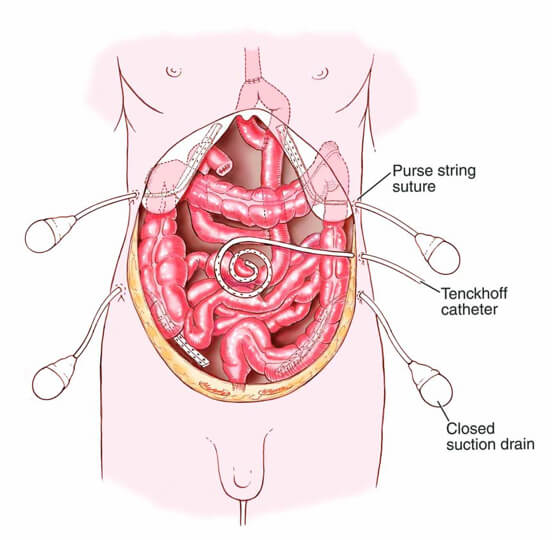
Β. Early postoperative intraperitoneal chemotherapy
The method may be used either alone as an adjuvant following tumor resection or in combination to hyperthermic intraperitoneal intraoperative chemotherapy provided the surgeon has assessed that it is required for microscopic tumor eradication.
Four drains are placed in the abdominal cavity (2 under the hemidiaphragms and 2 in the pelvis) and one Tenckhoff catheter for drug instillation.